
Meniscal Injuries: What Patients Really Need to Know
Meniscal injuries are common knee problems. Most people recover well without surgery, especially degenerative tears. The meniscus is cartilage that protects your knee, absorbs shock, and helps it move smoothly. Injuries often happen from twisting, pivoting, sports, or wear-and-tear over time. Some tears — like bucket-handle or root tears — may require surgery if they cause locking or instability. Early care includes relative rest, gentle movement, ice for pain, and elevation if swollen. Recovery usually takes 6–12 weeks for daily activities, longer for athletes, with ongoing improvement for up to a year. Supplements like vitamin D, omega-3s, or collagen may help but do not replace rehabilitation — see my home rehab exercises for meniscal injuries for step-by-step guidance. Understanding your injury improves recovery and reduces anxiety.
What is the meniscus and why is it important?
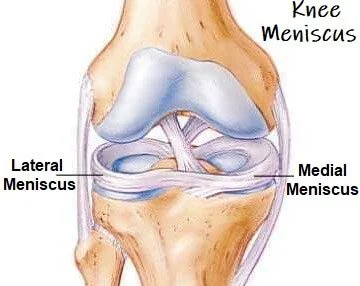
The meniscus is a crescent-shaped piece of cartilage in the knee that helps absorb shock, spread load, and protect joint cartilage during everyday and sporting activities [1]. Each knee has two menisci — a medial (inner) and lateral (outer) one.
The meniscus also contributes to joint stability and smooth movement, particularly during bending and twisting [2]. When meniscal tissue is lost or removed, stress on knee cartilage increases, raising the long-term risk of osteoarthritis [3].
Who gets meniscal injuries and how do they happen?
The medial meniscus is injured more often because it is less mobile and more firmly attached to the knee [2].
Meniscal injuries generally fall into two groups:
Traumatic tears, more common in younger, active people, usually caused by twisting or pivoting on a bent knee [4]. Sports with higher risk include football, rugby, basketball, and skiing [4].
Degenerative tears, common after age 40, often occurring without a clear injury during everyday movements such as squatting or kneeling [5]. These are most frequent between 45 and 65 years of age [5].
Some tear types are more specific:
Meniscal root tears most often affect the posterior root of the medial meniscus and are more common in middle-aged women and people with higher body weight [6].
Lateral meniscus tears occur more frequently alongside ACL injuries [7].
Which meniscal injuries are more likely to need surgery?
Most meniscal tears do not automatically require surgery, but some are less likely to settle with rehabilitation alone:
Bucket-handle tears can cause true locking of the knee when a fragment flips into the joint and often need surgery to restore movement [8].
Meniscal root tears occur where the meniscus attaches to bone [6]. When a root tears, the meniscus can no longer absorb load properly, making the knee function similarly to having no meniscus at all [6].
Large, unstable traumatic tears in younger people may be surgically repaired to protect long-term knee health [9].
These injuries are commonly caused by twisting under load, deep squatting, or high-impact sports injuries, particularly when combined with ACL damage [8,9].
Many meniscal tears do not need surgery
High-quality studies show that around 60–70% of degenerative meniscal tears can be managed successfully without surgery [10,11]. Exercise-based rehabilitation often produces similar long-term outcomes to surgery, without the risks associated with an operation [10–12].

Practical tip: Following a structured program can improve recovery. Start safely with my home rehab exercises for meniscal injuries to regain strength and mobility.
What to do in the first 24–48 hours after injury
Early management can influence recovery:
Relative rest is important, avoiding deep knee bending, twisting, or pivoting initially [13].
Gentle movement should usually begin within 24–72 hours, as pain and swelling allow [14].
Ice can help with short-term pain relief, but it does not speed healing and excessive use may interfere with tissue repair [13].
Anti-inflammatory medications, particularly at higher doses early on, may reduce pain but can also blunt biological signals needed for healing [15].
Compression and elevation can help manage swelling [13].
How long does recovery take without surgery?
Recovery is often slower than people expect, but outcomes are usually good:
Most people notice meaningful improvement within 6–12 weeks, with average recovery for daily activities closer to 10–12 weeks [10–12].
Athletes typically need 8–16 weeks of structured rehabilitation before returning to sport, depending on demands and tear type [12].
Improvement may continue for 6–12 months as swelling settles, movement control improves, and pain sensitivity reduces [16].
When is an MRI useful — and when is it not?
MRI can be helpful, but timing matters. An MRI may be useful if pain or swelling persists beyond 6 weeks despite appropriate rehabilitation [17], if there are mechanical symptoms such as true locking [18], or if a traumatic injury causes rapid swelling within 1–2 hours, raising concern for ligament injury such as an ACL tear [19].
Signs of ligament injury include the knee giving way, instability, or being unable to continue activity after injury [19].
Importantly, many people recover well even when MRI scans look “severe”, and meniscal tears are common in pain-free knees, especially with age [20]. MRI findings should guide decisions, but should not override symptoms and function [17–20].
Supplements and recovery
No supplement replaces rehabilitation, but some may support recovery:
Vitamin D: Blood levels above 50 nmol/L (20 ng/mL) are associated with better musculoskeletal health, with typical supplementation of 800–2000 IU per day depending on baseline levels [21].
Omega-3 fatty acids: Doses of 2–3 g per day of EPA+DHA have been used in studies examining joint inflammation [22].
Collagen or gelatin with vitamin C: Commonly 15 g collagen or gelatin plus ~50 mg vitamin C, taken about one hour before exercise [23]. These two are also useful for helping low back discs heal.
New research: why timing of rehab matters
Recent studies show meniscal healing is influenced by when and how load is applied [24]. Early, controlled loading within the first 1–2 weeks supports healthier biological healing than prolonged rest [24].
Why understanding your injury helps
Patients who understand their injury tend to have better expectations, stronger rehabilitation adherence, and higher satisfaction with care [25]. Education reduces fear, improves decision-making, and lowers the likelihood of unnecessary surgery [25].
Key takeaway
Most meniscal injuries recover well with the right rehabilitation, patience, and guidance. Surgery is sometimes necessary, but often avoidable — and understanding your injury is a powerful part of recovery.
Clinical Disclaimer
This information is for educational purposes only and is not a substitute for professional medical advice. Always consult a qualified healthcare professional for diagnosis, treatment, or questions about your specific condition.
Cliff Russell , Registered Osteopath @ Osteo Studio
References
Makris, E.A., Hadidi, P., Athanasiou, K.A. (2011). The knee meniscus: Structure–function, pathophysiology, current repair techniques, and prospects for regeneration. Biomaterials, 32(30), 7411–7431.
Fox, A.J., Bedi, A., Rodeo, S.A. (2012). The basic science of human knee menisci: Structure, composition, and function. Sports Health, 4(4), 340–351.
Papalia, R., et al. (2011). Meniscectomy as a risk factor for knee osteoarthritis. Journal of Orthopaedics and Traumatology, 12(4), 227–233.
Englund, M., et al. (2008). Incidence and risk factors of meniscal tears in young adults. Arthroscopy, 24(3), 308–314.
Beaufils, P., et al. (2014). Degenerative meniscus tears: Management and prognosis. Knee Surgery, Sports Traumatology, Arthroscopy, 22(3), 499–515.
LaPrade, R.F., et al. (2014). Posterior meniscal root tears. American Journal of Sports Medicine, 42(12), 3016–3030.
Magnussen, R.A., et al. (2012). Meniscus injury patterns with ACL tears. American Journal of Sports Medicine, 40(3), 516–523.
Beaufils, P., et al. (2017). Bucket-handle meniscus tears: Diagnosis and surgical approach. Orthopaedics & Traumatology: Surgery & Research, 103(1), 15–23.
Krych, A.J., et al. (2010). Repair of large meniscus tears. Sports Health, 2(2), 106–113.
Sihvonen, R., et al. (2013). Arthroscopic partial meniscectomy versus exercise therapy for degenerative meniscal tears. New England Journal of Medicine, 369, 2515–2524.
Katz, J.N., et al. (2013). Surgery versus physical therapy for meniscal tears in middle-aged and older adults. New England Journal of Medicine, 368, 1675–1684.
van de Graaf, V.A., et al. (2018). Exercise therapy for meniscal tears: Long-term outcomes. Arthroscopy, 34(5), 1552–1560.
Bahr, R., et al. (2017). First 48 hours after knee injury: Practical advice. British Journal of Sports Medicine, 51(13), 950–956.
Roos, E.M., et al. (2015). Early controlled loading in meniscal injuries. Clinical Rehabilitation, 29(5), 471–482.
Warden, S.J. (2010). NSAIDs and tissue healing. Sports Medicine, 40(6), 513–533.
Beattie, P.F., et al. (2008). Long-term functional recovery after meniscus injury. Journal of Orthopaedic & Sports Physical Therapy, 38(9), 524–533.
Roos, E.M., et al. (2008). MRI timing for meniscus evaluation. Osteoarthritis and Cartilage, 16(2), 142–148.
Beaufils, P., et al. (2010). Mechanical symptoms and meniscus tears. Knee Surgery, Sports Traumatology, Arthroscopy, 18(2), 197–204.
Papalia, R., et al. (2011). Ligament injuries with meniscus tears. British Journal of Sports Medicine, 45(5), 386–394.
Sihvonen, R., et al. (2016). Degenerative meniscus tears on MRI in pain-free adults. Annals of Internal Medicine, 164(7), 457–464.
Barker, T., et al. (2013). Vitamin D and musculoskeletal health. Journal of Clinical Endocrinology & Metabolism, 98(6), 2430–2437.
Simopoulos, A.P. (2002). Omega-3 fatty acids and joint health. Biomedicine & Pharmacotherapy, 56(8), 365–370.
Shaw, G., et al. (2017). Collagen supplementation and connective tissue. Current Medical Research and Opinion, 33(6), 1–10.
2024 Molecular meniscal mechanobiology studies. Journal of Orthopaedic Research, 42(2), 290–301.
Teunis, T., et al. (2014). Patient education improves meniscus rehabilitation outcomes. Knee Surgery, Sports Traumatology, Arthroscopy, 22(3), 594–601.